We know from research that health status is influenced by multiple factors including genetics, social circumstances, environmental exposures, health care, and behavioral patterns. What we might not fully realize is that behavioral patterns have the single greatest influence on personal and population health. This means that achieving better health at lower cost will require improvements in health promotion and prevention at the community level. The 3-4-50 framework can be a helpful tool for focusing these strategies.
3-4-50: A Focusing Framework for Community Health Improvement
The 3-4-50 Framework
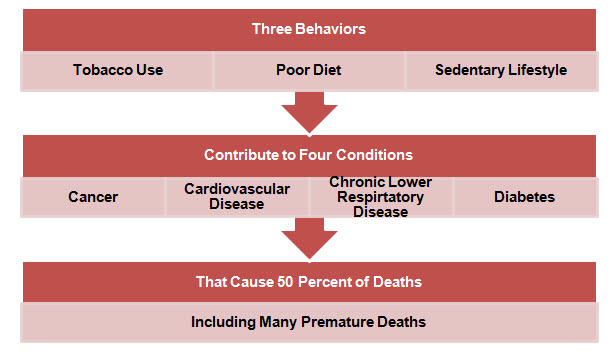
3-4-50 is a community health improvement strategy based on evidence that three health behaviors elevate risk for four chronic conditions that together cause more than fifty percent of deaths, including early deaths.
- The three health risk behaviors are unhealthy diet, sedentary lifestyle, and tobacco use.
- The four chronic conditions are cardiovascular disease, cancer, chronic lower respiratory disease, and diabetes.
- These four conditions cause more than 50 percent of all deaths in that vast majority of communities.
We know from research and experience that our health behaviors can be influenced by the environments where we live, learn, work, and socialize. Accordingly, community health interventions work best when we are able to create collective impact by providing consistent supports for healthy behaviors across settings. 3-4-50 is designed to support collaborative community strategies that potentially engage:
- Individuals and families;
- Businesses and employers;
- Health care systems, insurers, and clinicians;
- Community, non-profit and faith-based organizations;
- Early learning centers, schools, colleges, and universities; and
- State and local government.
The 3-4-50 concept was originally developed in the U.K. by the Oxford Health Alliance in response to global concerns about chronic disease. The underlying concept of unhealthy behaviors elevating risk for chronic disease and early death were not new. What was new is an approach to framing the connections between these factors in the 3-4-50 model.
The Evidence for 3-4-50
The evidence indicates that the core elements of 3-4-50 are strikingly relevant in the US at the national, state, and community level. For example:
- There is strong evidence the 3-4-50 risk factors (individually or in combination) elevate risk for cardiovascular disease, cancer, chronic lower respiratory disease, and diabetes in the U.S. (see evidence profiles for nutrition, physical activity, tobacco, cardiovascular disease, cancer, chronic lower respiratory disease, and diabetes in HealthyPeople.gov).
- The 3-4-50 diseases do account for 50 percent of total deaths (including early deaths) in the vast majority of communities.
- There are many evidence-based interventions consistent with 3-4-50 that can be implemented in the community, the clinic, the school, and the workplace.(Community Preventive Services Task Force, US Preventive Services Task Force).
- Assuming evidence-based interventions are effectively implemented, the near-term (1-2 year) impact of a 3-4-50 approach should include better health behaviors, better screening rates, and improvements in clinical indicators related to each disease. There may also be improvements in health service utilization and reductions in preventable hospital utilization for some higher risk populations.
- The longer-term impacts on disease rates, death rates, and health spending can be predicted based on evidence that populations with healthier lifestyles tend to live longer and spend less on preventable conditions. Even marginal reductions in disease development can have a substantial impact on health and economic indicators over time.
3-4-50 Interventions
3-4-50 interventions can be implemented at the community level, program level, or individual level. A cross-section of examples could include:
- Helping people recognize and make healthy food and beverage choices
- Increasing access to healthy and affordable foods in communities
- Implementing organizational and programmatic nutrition standards and policies
- Assuring food safety and improving nutritional quality of food supply
- Supporting policies and programs that promote breastfeeding
- Assessing physical activity levels and providing education, counseling, and referrals
- Supporting workplace policies and programs that increase physical activity
- Facilitating access to safe and affordable places for physical activity
- Encouraging community design and development that supports physical activity
- Promoting and strengthening school and early learning policies and programs that increase physical activity
- Supporting comprehensive tobacco free and other evidence-based tobacco control policies
- Expanding use of tobacco cessation services
- Using media to educate and encourage people to live tobacco free
Initiatives like these can be implemented community-wide or within particular settings (e.g. health care, schools, or workplace). They can also be focused on the general population or on special populations with particular needs (e.g. children, seniors, medically underserved, persons with disabilities).
3-4-50 examples from the field
The 3-4-50 framework has been flexibly adapted in multiple settings. The most prominent documented examples include:
In both of these settings, 3-4-50 is applied as an organizing framework to help communities focus on the connections between risk behaviors, chronic disease, and early death. The underlying health science is not new. The innovation is in the framing of the message, and the mobilization of effort in response to the message.
Strategy and Technical Support for 3-4-50 Projects
Community Health Solutions is offering support for design and implementation of 3-4-50 projects. We envision the typical 3-4-50 project as a Action Learning Network with multiple participating organizations, and one or more sponsors. Our role is to provide strategy advice and technical support to help stakeholders:
- Assess population health status and health risk behaviors;
- Define 3-4-50 improvement objectives;
- Design 3-4-50 improvement strategies;
- Build capacity for implementation and evaluation; and
- Execute for results.
Our special capabilities for this work include:
- Extensive experience in designing and managing community health improvement collaboratives;
- Unique capabilities in data development, best practice research, capacity building, execution support, and evaluation;
- Unique capabilities in web-based performance support that allow multiple organizations to streamline the process of learning, capacity building, execution, and evaluation.
Investing in 3-4-50 Projects
An investment in a 3-4-50 project is an investment in population health improvement at the community level. Accordingly, investors in a 3-4-50 project could potentially include employers, foundations, hospitals, health systems, health plans, public agencies, schools, and other community-based organizations. Some points to consider for potential investors include:
- A 3-4-50 project can be started with a large group of collaborating partners, or just one or two organizations. In the latter case, once the initiative is established, additional partners can be added over time.
- 3-4-50 is not an ‘all or nothing’ strategy. It is a flexible strategy based on a portfolio of evidence-based practices. 3-4-50 can be aligned to reflect the particular values of communities, clinicians, employers, schools, etc.
- A 3-4-50 project need not be highly expensive, especially on a per-capita basis. Typically there are a series of low-cost interventions related to policy and practice change which can be implemented right away. These interventions can be scaled at a decreasing marginal cost. More substantial investments in large-scale communications or the built environment, if needed at all, can be made on a collaborative basis after substantial planning.
- A 3-4-50 project need not be exclusive of other community health priorities. 3-4-50 is inclusive of vulnerable populations and special needs populations. 3-4-50 is also compatible with initiatives focused on mental health, oral health, maternal and infant health, and other community priorities.
Getting Started
Getting started on a 3-4-50 project is as easy as a phone call or email. Contact Steve Horan at 804.673.0166 or shoran@chsresults.com for a no-obligation consultation about the potential for a 3-4-50 project in your community.
